
A massive transformation just swept across the landscape of American public health, not because of a sudden change in lifestyle, but due to a pen stroke in medical methodology. Millions of citizens who went to bed classified as merely “overweight” are now technically considered clinically obese under a progressive diagnostic framework developed in Europe.
The new system, engineered by the European Association for the Study of Obesity (EASO), introduces a multi-tiered approach. It no longer relies strictly on the numbers on a traditional weight scale. Instead, it integrates existing metabolic complications—such as high blood pressure, joint issues, or fluctuating blood sugar levels—directly into the primary diagnosis. For a nation already wrestling with metabolic health challenges, this systemic update serves as a profound reality check, shifting the domestic data points in a way that forces us to question how we define wellness.
Unpacking the Numbers: The 12.2% Statistical Leap
According to a comprehensive study featured in the Annals of Internal Medicine, applying this updated diagnostic lens to the United States produces staggering results. Roughly one in every five American adults previously tucked into the “overweight” bracket has been reclassified. This structural adjustment instantly inflates the national obesity statistic from an already concerning 42.4% to an unprecedented 54.2%.
U.S. Obesity Rate Comparison:
- Standard BMI Model: 42.4%
- New EASO Framework: 54.2%
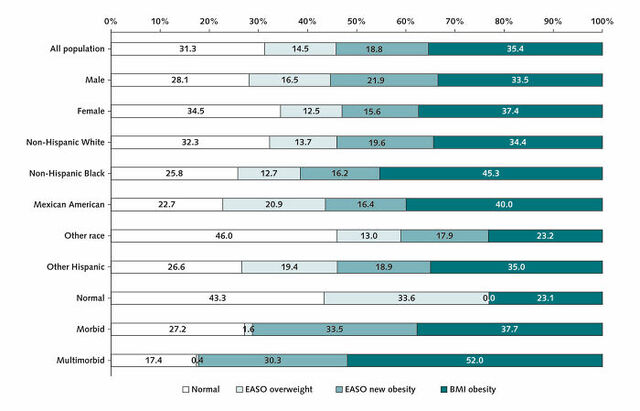
To map out this shift, investigators analyzed long-term tracking data encompassing more than 44,000 participants from the National Health and Nutrition Examination Survey (NHANES) spanning nearly two decades. Under the classic, single-step assessment, the baseline breakdown of the cohort positioned 35.4% as obese, 33.3% as overweight, and 31.3% within a medically optimal range. However, when the dual-layered criteria were introduced, the internal dynamics changed dramatically. The data revealed that the individuals migrating into the redefined category skewed older—averaging 51.3 years of age compared to the 36.5-year average of those remaining in the traditional overweight tier. Adult men and individuals already managing chronic physiological strain were also significantly more likely to be swept into this expanded clinical definition.
Watch the comprehensive breakdown of this public health emergency in the video Obesity in America: a Nation’s Health Crisis below.
The Deficiencies of a Single Metric: Why Weight Ratios Miss the Mark
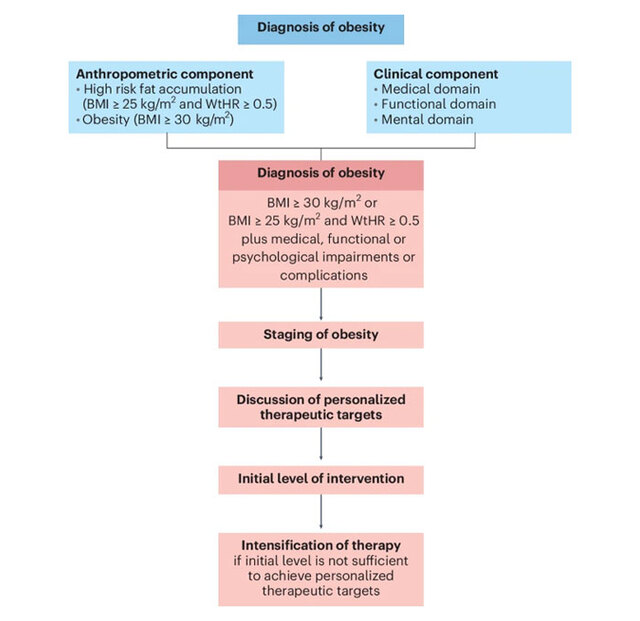
For generations, the Body Mass Index (BMI) has reigned supreme as the gatekeeper of metabolic assessment. Calculated purely by dividing a person’s weight by the square of their height, it provides a quick, uncomplicated numerical value. Anyone landing a score of 30 or above is labeled obese, while those sitting between 25 and 29.9 are deemed overweight.
The core flaw of this legacy framework is its complete blindness to body composition and internal wellness. It treats pounds of dense athletic muscle and pounds of adipose tissue as completely identical, frequently miscategorizing active individuals while ignoring vulnerable patients who carry dangerous visceral fat beneath an otherwise average exterior.

The European model remedies this oversight by keeping the initial BMI threshold but immediately executing a critical secondary evaluation. If a patient falls into the 25 to 29.9 range but presents even one weight-aggravated medical issue, the condition is upgraded to clinical obesity. Among the reassessed American demographic, a striking 57.5% suffered from at least one such chronic ailment. Chronic high blood pressure emerged as the most dominant contributor, impacting 79% of the newly categorized group. Joint inflammation and degenerative arthritis followed at 33.2%, while advanced blood sugar imbalances and diabetes accounted for 15.6%.
Expanding Patient Access to Preventative Interventions

While seeing a national health metric surge past the halfway mark is jarring, healthcare professionals point out that broadening these definitions carries massive long-term advantages. The primary benefit lies in dismantling the rigid institutional barriers that block patients from receiving early care.
“The new EASO framework may provide a more sensitive tool to diagnose obesity than the traditional BMI definition,” the researchers noted, signaling a vital shift toward holistic patient management.
Currently, insurance providers and medical networks rely strictly on a high BMI cutoff to authorize advanced weight-management therapies or coverage for modern metabolic medications like Ozempic. By acknowledging that a slightly lower weight accompanied by severe hypertension poses an equal—if not greater—danger, the new standard could grant millions of vulnerable individuals access to life-altering pharmaceutical and therapeutic interventions before irreversible systemic damage occurs.

Red Flags: Premature Mortality and the True Cost of Neglect
The urgency behind this diagnostic shift is driven home by a sobering reality: survival rates. When researchers monitored the long-term outcomes of the individuals newly added to the obesity category, they discovered a 50% higher risk of premature death compared to peers maintaining an optimal baseline weight.
To understand the severe health complications driving this mortality spike, the internal medical data reveals a striking distribution of chronic illnesses within this newly reclassified demographic:
- High Blood Pressure (Hypertension): Affects 79.0% of the group, standing as the single most dominant cardiovascular threat.
- Arthritis / Joint Degeneration: Affects 33.2% of individuals, highlighting the severe structural and physical toll on the body.
- Diabetes / Metabolic Imbalance: Affects 15.6% of the population, marking a significant risk for systemic metabolic failure.
This statistical red flag elevates weight-related conditions to the same level of public health urgency as historic anti-smoking campaigns. Cardiovascular deterioration, arterial strain, and accelerated cellular aging mean that carrying excess fat alongside metabolic issues is a quiet catalyst for critical illness. Redefining the terminology isn’t about cosmetic labeling; it’s a vital effort to intercept severe chronic illness before it turns fatal.

The Public Disconnect: Netizens Debate Culture, Lifestyle, and Medical Standards
As the study made its way across digital spaces, it ignited a fiery debate regarding western lifestyles, systemic corporate food production, and personal accountability. Many online commenters focused on the cultural contrasts in diet and urban design between continental Europe and the United States.
Many point out that the domestic landscape is fundamentally built around hyper-processed convenience foods, car-dependent infrastructure, and a lack of baseline nutritional education. One commenter noted the stark cultural shift experienced when traveling internationally, observing how standard communities abroad prioritize pedestrian movement and local, unrefined ingredients. Others expressed concern that modern parenting trends risk normalizing these metabolic imbalances early on, inadvertently setting children up for severe long-term cardiovascular risks.

At the same time, a significant portion of the public viewed the shifting guidelines with skepticism. Some argued that medical institutions are simply “moving the goalposts” to expand the consumer base for expensive lifelong pharmaceuticals. The classic defense regarding athletic body types emerged frequently, with individuals noting that robust muscle mass regularly breaks traditional metrics. However, medical counterarguments emphasize that regardless of whether extra mass stems from adipose tissue or extreme weight training, an overgrown vascular network places an undeniable, long-term physical strain on the heart and skeletal joints.
Watch the full ABC News segment detailing the impact of this framework: Over 75% of US adults may meet criteria for obesity under new definition.
Final Thoughts: Global Policy and the Path Forward
At present, this diagnostic methodology remains a distinctly European initiative, with nations like Ireland and the Netherlands gradually weaving elements of the framework into their local medical networks. Major global entities like the World Health Organization (WHO) and federal agencies within the United States have not officially adopted the standard, keeping the traditional weight-to-height ratio as the baseline for medical records.
However, as the data connecting the updated framework to premature mortality continues to mount, a shift in domestic policy may become inevitable. Transitioning from an arbitrary weight scale to a holistic, health-first diagnostic system could rewrite how healthcare providers manage preventative wellness. By treating weight not as an isolated cosmetic metric, but as an interconnected component of internal metabolic stability, the medical community can finally move away from reactive treatments and focus on true, proactive prevention.


